Partner With Us
We welcome all healthcare professionals including medical doctors, osteopaths, naturopaths, chiropractors, nurse practioners, physician assistants and more. If you are interested in using PotassiMax to support your patients' health, complete this contact form and we'll reach out to you with a simple get-started package.

Healthcare professionals
PotassiMax partners with like-minded physicians and other healthcare practitioners who want to treat the root cause of hypertension and other age-related diseases.
Through our patient-referral program, PotassiMax supports medical practices and contributes to enhancing the primary care experience.
If you are interested in recommending PotassiMax to your patients, contact us using the form below.
Section 1: Epidemiology
Population studies in the U.S. and around the world show that potassium deficiency is widespread.
Median daily intake in the U.S.
2,300mg daily

Potassium Excretion (g/day)
NHANES 2003–2018, 13,855 participants
Source: NEJM 2014; 371(7): 612
Median daily intake across 17 countries
2,000mg daily

Potassium Intake (mg)
101,945 patients from 17 countries
Source: BMC Public Health (2024) 24:180
Most of your patients are deficient in potassium relative to expert guidelines
2,300 mg
Average American
In a study of 12,000 Americans, less than 2% got the amount of potassium recommended by experts. The average intake was only 2,300 mg per day

4,700 mg
Recommended daily intake
- American College of Cardiology 5,000 mg daily
- National Kidney Foundation 4,700 mg daily
- Food & Drug Administration 4,700 mg daily
Section 2: Mechanism of Action
Clinical research shows us that potassium controls blood pressure through two discrete mechanisms
1. Down-regulation of the Renin-Angiotensin-Aldosterone System (RAAS)
Human intervention trials show that increasing daily urinary potassium excretion to 100 mmol (3,900 mg) can supress renin secretion. Decreases in renin downregulate the RAAS, leading to increased excretion of sodium and water.
As potassium intake increases, renin secretion decreases
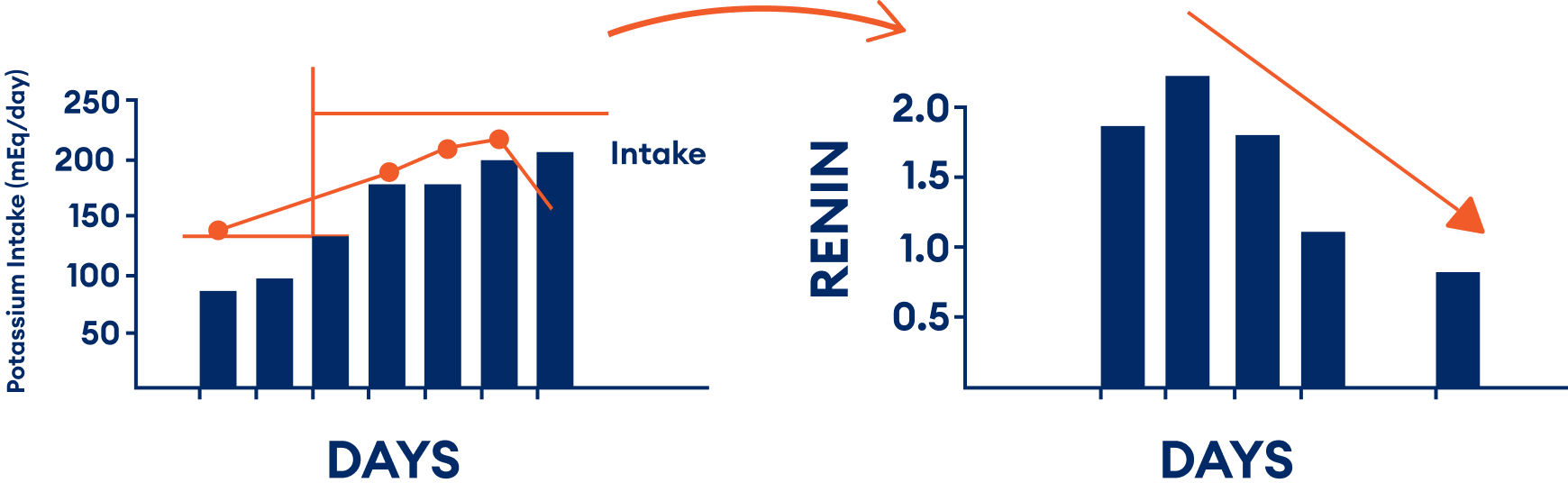
Source: Brunner et al. The Influence of Potassium Administration and of Potassium Deprivation on Plasma Renin in Normal and Hypertensive Subjects. The Journal of Clinical Investigation 1970;49: 2128-2138
Source: Maebashi, M., Y. Miura, and K. Yoshinaga. 1968. Suppressive effect of potassium on renin release. Jap. Circ. J. 32: 1265.
Source: Veyrat, R., H. R. Brunner, E. L. Manning, and A. F. Muller. 1967. Inhibition de l'activite de la renine plasmatique par le potassium. J. Urol. Nephrol. 73: 271.
Excerpt from the 2017 ACC/AHA Task Force on Clinical Practice Guidelines
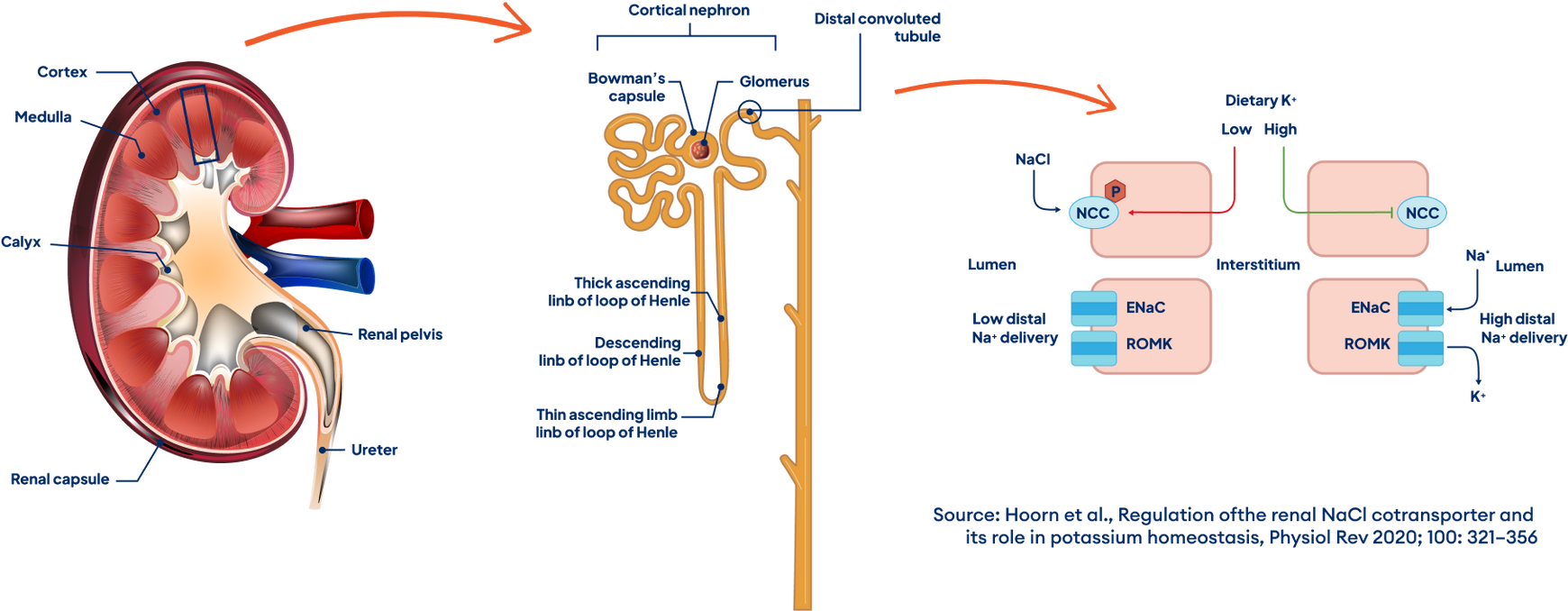
2. Dephosphorylation of the Sodium Chloride Co-transporter (NCC)
The NCC in the distal tubule acts to retain sodium, chloride and water when in its phosphorylated active state. Low dietary intake of K triggers the phosphorylation of NCC, while higher intakes of K result in dephosphorylation of the NCC, allowing for the excretion of excess sodium and water.
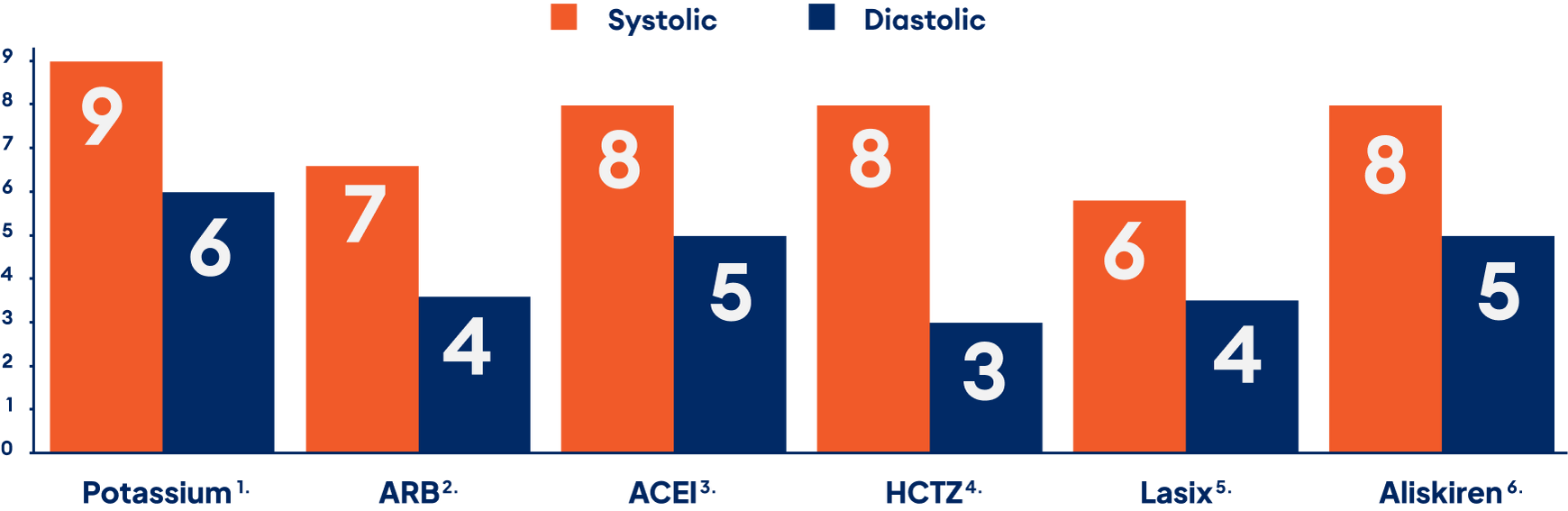
Section 3: Efficacy
Potassium supplementation has similar effect to medications that target the RAAS


Contact Us
Have a question or comment? We would love to hear from you. Fill out this form or reach out via phone or email. We're all ears!